




The world is experiencing an unprecedented period of global health challenges. Times of emergency require radical choices, but also offer opportunities for course correction and innovative thinking. Making good policy choices during a crisis relies on understanding past choices and their impact to avoid repeating past mistakes. The past 40 years in global health policy offer lessons on cause and consequence, which global leaders should heed.
Global health ‘trends’ and (unintended) consequences
The 1978 Alma Ata Declaration enshrined principles of human rights, equity, and participation, with primary health care as the driver of Health for All. Early progress was undone by the structural adjustment programs of the late 1980s and 90s that prioritized economic reform, reduced public spending, and applied business principles to health care.
Following the recognition of the harmful effects of low-income country debt and chronic underinvestment in social services, including health, the Millennium Development Goals in 2000 focused on poverty elimination in low-income countries and coalescing around a narrow set of health priorities including disease prevention through specific global funding initiatives. This period was characterized by large-scale, intervention-focused vertical programs, delivering drugs, vaccines, and therapeutics against malaria, AIDS, neglected tropical diseases, and other infections for billions of people.
However, this focus on output to the exclusion of quality, accessibility, acceptability, affordability, and availability of services had unintended consequences.
Emphasizing simple, easy-to-count commodities such as drugs, vaccines, and bed nets, led to the neglect of comprehensive environmental and behavioral measures; vertical funding made it difficult to plan and fund comprehensive health care services; resourcing of specialized staff and clinics, as with HIV/AIDS, decimated primary health care services; and countries were incentivized to target easy-to-reach populations while inequalities worsened.
We need a fundamental commitment to shifting power dynamics and structural barriers in pursuit of a multi-sectoral and equity-focused approach to health.
—One step forward, two steps back?
From 2015, the 2030 Agenda for Sustainable Development and its associated 17 Sustainable Development Goals began to undo the damage by focusing on equity, universal health coverage, and cross-sectoral collaboration for people, the planet, and prosperity. There are positive signs, such as within the UHC movement, of a shift toward redressing the funder-recipient power imbalance. WHO NTD road map 2021-2030, published in January 2020, with its focus on country ownership and multi-sectoral approaches is an example of this shift.
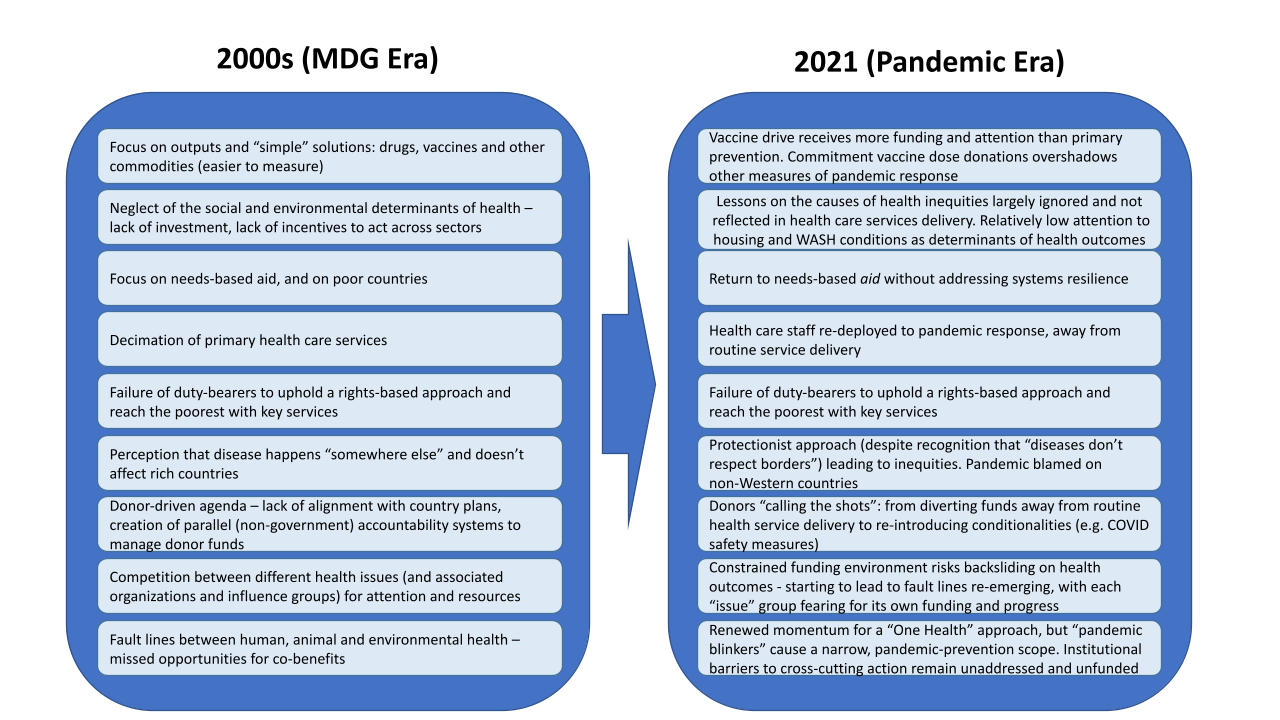
Worryingly, this positive trend is at risk following the COVID-19 pandemic, with a return to MDG-era practices such as prioritization of easy-to-measure commodities, protectionism of donor country interests, and aid conditionalities — all of which contrast with the recent decade’s move toward strengthening health systems. The figure below provides a thorough examination of the striking similarity between the current situation and the MDG period:
The crossroads
As countries balance third-wave responses with efforts to rebuild their economies and health systems, there are opportunities for ambition. The recent G-7 summit was the first in a series of such opportunities, including several G-20 meetings and discussions on a global pandemic prevention and preparedness treaty, among others. Based on past lessons, the global community is evidently faced with two clear paths:
1. The recent cuts to U.K. official development assistance, including a whole range of programs crucial to global health — including water and sanitation; polio eradication, and UNAIDS, to name just a few — demonstrate this risk. “Emergency mode” leads to earmarked funding toward funder-led priorities, and political pressure to deliver on pandemic response risks a return to easy-to-measure output to the detriment of system reforms and addressing the social and environmental determinants of health and health inequities.
2. This could be the era in which intersectoral approaches are truly adopted, and investment is made in the services which have far-reaching, long-term impacts. A new report by WaterAid has shown that achieving the U.N. targets on sanitation, for example, could prevent up to 6 billion cases of diarrhea and 12 billion cases of parasitic worms between 2021 and 2040. This highlights the importance of a One Health approach within health funding and delivery.
Opinion: Global health security must be tied to health systems
Building back better means reimagining global health investments in bold new ways. Integration, financing, and equity must all be at the heart of this work.
The revitalization of the global health architecture can be bolstered by recent efforts to address entrenched power structures while strengthening global bodies such as the World Health Organization. Above all, this path builds on the recognition of country ownership as fundamental to improving health outcomes and national, regional, and global health systems’ resilience.
It’s not too late
Global leaders can still chart a new course for global health, by committing to:
• A fully-funded, stronger WHO that makes its own decisions based on global priorities.
• A comprehensive, well-funded global One Health architecture that identifies and prevents future risks.
• Global health solidarity through a binding global health treaty that provides for integrated approaches on WASH, housing, livelihood, animal health, and environmental services.
• Using emergency preparedness as an opportunity to strengthen health systems and country ownership.
• Addressing the social and environmental determinants of health, including building and maintaining infrastructure to support universal access to WASH, through appropriate financing for intersectoral coordination. For example, by investing about $6.5 to 9.6 billion needed between 2020 and 2030 to establish basic water services in health care facilities in 47 least-developed countries.
As NGOs, we know we must demonstrate good practice to redress the power imbalance that reinforces inequalities. SCI Foundation and WaterAid both put systems strengthening and country plans at the heart of our efforts. We know which of the above paths we would choose, but “walking the talk” of this aspiration considering current events, the recent cuts to U.K. aid and disappointing G-7 outcomes will be difficult.
We need a fundamental commitment to shifting power dynamics and structural barriers in pursuit of a multi-sectoral and equity-focused approach to health. Getting there will take leadership, political commitment, and financing to set the global health community on a transformative course.
We hope leaders share our vision as they decide which path to take.
Visit the Building Back Health series for more coverage on how we can build back health systems that are more effective, equitable, and preventive. You can join the conversation using the hashtag #BuildingBackBetter.

About the authors

Yael Velleman
Yael Velleman is the director of policy and communication at the SCI Foundation and has worked with the organization since 2018. She is passionate about making the world a cleaner and healthier place for all, with a particular interest in the links between WASH and public health and has worked extensively on strategic planning and policy engagement on WASH and neglected tropical diseases. She has worked in the U.K., Uganda, and Nicaragua, and has supported work in several countries in sub-Saharan Africa and Asia.
Helen Hamilton
Helen Hamilton is a senior policy analyst on health and hygiene at WaterAid. She has been working at WaterAid since 2017. Helen leads the organization’s policy analysis and advocacy on global health and hygiene, championing policy, programming and research innovation on comprehensive approaches to public health. Her experience includes linking WASH aspects with programs to improve maternal and newborn health, quality and safety of care, and working to strengthen health systems governance and approaches to infectious diseases and inclusion and equity.



